On Thursday, Vertex Pharmaceuticals (VRTX) announced results from a phase 3 trial addressing whether ivacaftor would be effective in the treatment of the R117H mutation:
The mean absolute treatment difference in the change from baseline in percent predicted FEV1 between treatment with ivacaftor and placebo was 2.1 percentage points (p=0.20) and the mean relative treatment difference in percent predicted FEV1 was 5.0 percent (p = 0.06) through the 24-week treatment period among all patients (intent-to-treat analysis). The study did not meet its primary endpoint of the absolute change from baseline in FEV1 (percent predicted forced expiratory volume in one second, FEV1) throughout the treatment period for ivacaftor compared to placebo across all patients. A pre-specified subset analysis in patients 18 years of age and older (n=50) showed statistically significant improvements in lung function and other key secondary endpoints. In these patients, the mean absolute treatment difference in percent predicted FEV1between treatment with ivacaftor and placebo was 5.0 percentage points (p=0.01) and the mean relative treatment difference in percent predicted FEV1 was 9.1 percent (p=0.008) through the 24-week treatment period.
This article discusses the implications of the above clinical trial results.
Cystic fibrosis is one of the most common severe genetic disorders. When it was first described in 1938, life expectancy for patients with cystic fibrosis was approximately 6 months. With modern standard-of-care therapy, life expectancy is now around 35-40 years, although patients are frequently debilitated for much of that lifespan as multiple organ systems fail. The disease occurs when patients inherit two copies of mutated genes for the CFTR, a chloride channel essential for maintaining proper viscosity in mucus and other secretions. Over 1500 different mutations in the CFTR, although a few account for the vast majority of cases, with the most common being deletion of phenylalanine-508. The severity of a patient's symptoms depends on how much residual CFTR function they have, with the degree of residual function (if any) dependent on the mutations present in that particular patient's genome.
Vertex Pharmaceuticals is a clinical-stage biotech with an unchallenged lead in the treatment of cystic fibrosis. At present, Vertex has one drug approved for CF, Kalydeco (ivacaftor), which is currently approved for the treatment of patients with the G551D mutation in the cystic fibrosis transmembrane conductance regulator (CFTR). Substantially all of the patients with the G551D mutation in the developed world are already being treated with Kalydeco, for annual revenues of $400 million. The company is currently performing clinical trials to expand the label to include patients with other gating/residual function mutations such as R117H.
(click to enlarge)
The R117H mutation is a class IV residual function mutation in the CFTR. About 1% of all patients with cystic fibrosis have at least one R117H mutation, with the exact percentage varying from population to population. Vertex claims that the average life expectancy for patients with R117H is in the 50s.
In 2009, researchers in France obtained data on 95% of the French patients known to possess the R117H/delta-F508 combination. Sweat chloride levels 30 mM and higher were present in 50-70% of the patients, but sweat chloride levels did not correlate with clinical symptoms. Of the 72 children identified by newborn screening, 55 were asymptomatic and 17 were symptomatic. However, among 112 patients identified by means other than newborn screening (and older than the newborn-screening population), 103 had symptoms and 9 were asymptomatic. Among the 103 older symptomatic patients, the only symptom was infertility due to congenital absence of the vas deferens for 55 individuals. The remaining half had moderate to severe pulmonary disease or pancreatic manifestations of CF.
(click to enlarge)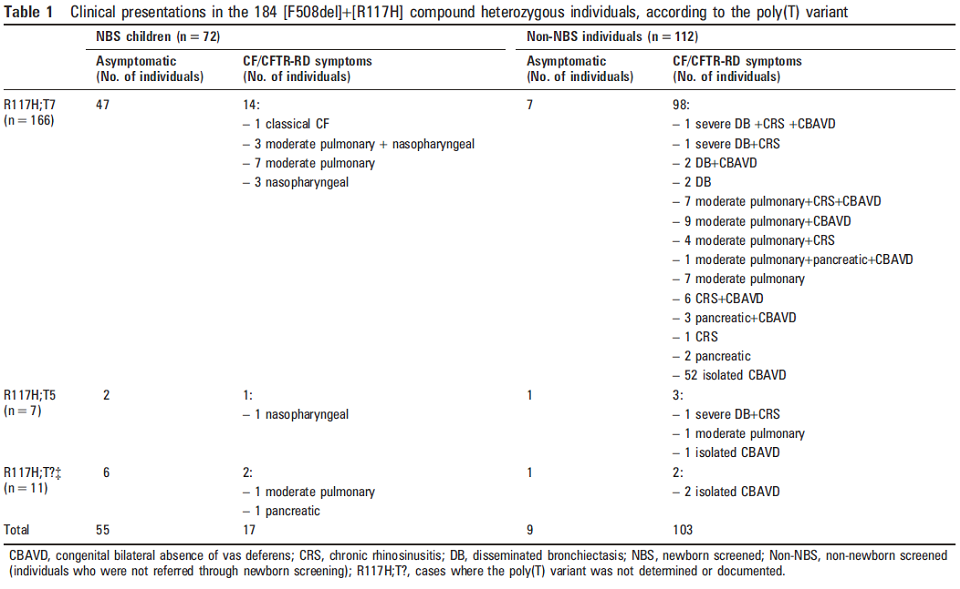
Based on delta-F508 and R117H allelic frequencies in the French population, the expected prevalence of CF due to a combined delta-F508/R117H genotype would be 3650 individuals. However, the French CF Laboratory Network had records of only 112 patients with this genotype and symptoms of CF. This discrepancy could be due to one or more of the following: many patients with the delta-F508/R117H genotype died young and were consequently underrepresented in current medical records; the patients were symptomatic but not diagnosed with cystic fibrosis; or the large majority of patients never developed significant disease attributable to cystic fibrosis. In France the high male:female gender imbalance, with many patients presenting due to infertility, suggests that the latter two causes probably dominate over the former. In other words, many patients with a genotype of delta-F508/R117H experience a relatively benign course. When pulmonary symptoms manifest, however, deterioration can be rapid.
The French results are probably the best available population-based data on the burden of disease due to R117H. Extrapolating from these findings, we can expect about 500 older patients in the developed world to have symptomatic R117H cystic fibrosis (of whom many will have a milder disease). There should also be about 400-500 patients in the developed world who are younger than 18 who will have R117H and will have some symptoms, although in many cases it will be unclear if those symptoms are truly attributable to CF as opposed to other respiratory ailments such as asthma or reactive nasopharyngeal polyposis.
In Vertex's recent trial on R117H, the failure to achieve statistical significance for FEV1 values can be attributed entirely to the heterogeneous patient population used in the study. Among patients over age 18, the average baseline FEV1 was 65% if the predicted value, indicating moderate underlying lung damage. These patients demonstrated a dramatic response to ivacaftor, with absolute FEV1 rising by 4.5 percentage points after 24 weeks of treatment (p = 0.002). Patients also reported excellent responses in terms of subjective respiratory symptoms (p < 0.0001). Among children aged 6-11 in the study, there was no significant change in FEV1 over the trial period (p = 0.132).
At the start of the study, however, these children had essentially normal FEV1 (96% of predicted). Consequently, it was impossible for the children to demonstrate improved FEV1 due to treatment even if disease progression was slowed or halted. It is not appropriate to consider this phase 3 trial as a failure when the results are muddied by the inclusion of patients with baseline normal FEV1.
(click to enlarge)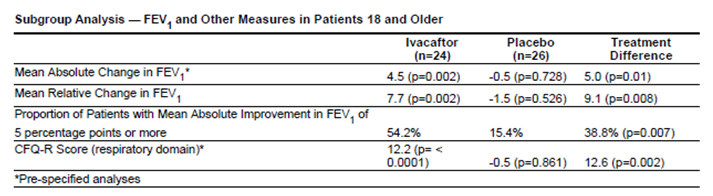
From these data, it is clear that older patients with R117H cystic fibrosis and significant lung damage benefit from ivacaftor. The FDA will probably approve ivacaftor for this patient population, yielding incremental revenues of $55-$70 million. Because there is almost no marginal cost to Vertex associated with marketing the drug to those patients, the R117H revenue will flow almost completely to the bottom line.
It's much less likely that the FDA will approve ivacaftor for asymptomatic people under 18 with an R117H genotype. As a radiologist who has interpreted chest CTs for R117H children, I can tell you anecdotally that even the asymptomatic or minimally symptomatic kids have abnormal lungs with signs of chronic damage. If I were the parent of an asymptomatic child with R117H, I would definitely want my child to take ivacaftor in order to prevent the disease from manifesting during adulthood. The FDA, however, is sensitive to economic and political factors and is aware that Vertex charges $300,000 per patient for Americans on ivacaftor.
Ivacaftor also carries a small risk of side-effects, most often a mild elevation in liver function tests. Because approving ivacaftor for people under 18 would create a significant economic cost without an obvious and immediate medical benefit, the FDA will probably not include asymptomatic young people on the expanded drug label. There will be a trivial amount of off-label use but few families will be able to find the cash to pay for the drug even if Vertex offers substantial subsidies. The meeting with the FDA to discuss the R117H data is scheduled for March 27th.
While R117H treats too few patients to have a material effect on Vertex's short-term value, the likely approval of ivacaftor for a subset of patients with the R117H mutation will slow the company's cash burn rate. As of the last quarter, the company lost $124 million against a net expendable cash of about $1 billion. Vertex estimates that there are about 5000 addressable patients with residual function mutations. Because many of these patients have rare mutations that will never be amenable to dedicated randomized trials, Vertex is performing a so-called "n of 1" clinical trial to see if this grab-bag of different patients is likely to benefit from ivacaftor therapy.
Using the R117H experience as a very loose prognosticator (the biology is obviously different), we can estimate that the yield on this entire patient pool will be around 50%, or about 2000 patients beyond the 500 new R117H patients who will become eligible for ivacaftor. In total, I expect the R117H and gating/residual function patients to yield $350 million for Vertex starting at the beginning of 2015.
With the current balance sheet, revenues from R117H and gating/residual function mutations will give Vertex about 3 years to move ivacaftor/lumacaftor/VX-661 triple therapy into the clinic before cash runs short. Thus, the real upshot from the latest clinical trial data is that Vertex will have the cash to develop next-generation combination therapy for the harder-to-treat delta-F508 homozygotes and heterozygotes who comprise 90% of the cystic fibrosis population. Estimates of the probability that ivacaftor/lumacaftor combination therapy will succeed in delta-F508 homozygotes vary considerably, from the 90% likelihood I offered in a previous article to somewhat lower estimates from other analysts. With the revenues gained from R117H and other low-prevalence residual function mutations, Vertex will have the funds for a second shot at the delta-F508 homozgyotes should the ivacafor/lumacaftor double combination fail.
Based on this new clinical data, I reiterate my conservative valuation of Vertex at $80 per share. When additional in vitro and physiologic data become available in the next few months, I will try to update this valuation before the pivotal TRAFFIC and TRANSPORT trials post results this coming summer.
Disclosure: I am long VRTX. I wrote this article myself, and it expresses my own opinions. I am not receiving compensation for it (other than from Seeking Alpha). I have no business relationship with any company whose stock is mentioned in this article. (More...)
Additional disclosure: Please perform your own due diligence prior to investing in this or any other security.
This entry passed through the Full-Text RSS service — if this is your content and you're reading it on someone else's site, please read the FAQ at fivefilters.org/content-only/faq.php#publishers.
Aucun commentaire:
Enregistrer un commentaire